Get Stop Work Immediately Doctor Referral Due To Pregnancy Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Stop Work Immediately Doctor Referral Due To Pregnancy Form online
Filling out the Stop Work Immediately Doctor Referral Due To Pregnancy Form online can be a straightforward process when guided step by step. This guide aims to provide clear instructions on how to accurately complete the form to ensure proper processing and support during your pregnancy.
Follow the steps to complete the form online for at risk pregnancy verification.
- Click ‘Get Form’ button to access the form and open it in your desired online editor.
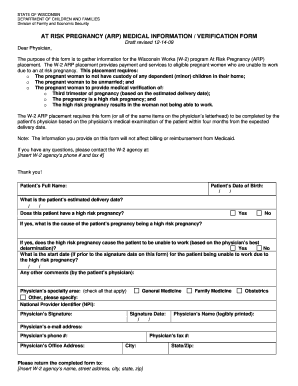
- Begin by entering the patient’s full name in the designated field at the top of the form.
- Next, input the patient’s date of birth using the provided date fields.
- Indicate the patient's estimated delivery date by filling in the required date fields.
- Select whether the patient has a high risk pregnancy by choosing 'Yes' or 'No'.
- If 'Yes' is selected, specify the cause of the pregnancy being high risk in the designated comments section.
- Declare whether the high risk pregnancy causes the patient to be unable to work by selecting 'Yes' or 'No'.
- If 'Yes', provide the start date for the patient's inability to work due to the high risk pregnancy.
- Add any additional comments by the patient’s physician in the comments section.
- Select the physician's specialty area by checking all applicable options.
- Enter the National Provider Identifier (NPI) of the physician.
- Have the physician sign in the designated space and include the signature date.
- Fill in the physician's office address along with the physician's fax number and city.
- Ensure the physician’s name is legibly printed, and provide their email address and phone number.
- Once all fields are completed, save any changes made, and choose to download, print, or share the form according to your needs.
Start filling out your forms online today to ensure timely processing and support.
To get excused from work while pregnant, you should have a candid discussion with your doctor about your health and any work-related challenges. Your doctor can provide guidance and may prepare a Stop Work Immediately Doctor Referral Due To Pregnancy Form if they believe you need time off. This documentation is vital for informing your employer and ensuring that your health needs are met.
Industry-leading security and compliance
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.