Get Mbf Smmp Claims Fax Number Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Mbf Smmp Claims Fax Number Form online
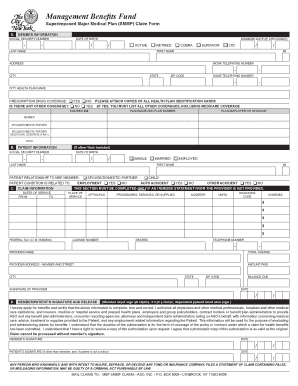
Filling out the Mbf Smmp Claims Fax Number Form online is a straightforward process that enables users to submit their claims for medical expenses incurred under the Superimposed Major Medical Plan. This guide offers clear and detailed instructions tailored to assist all users, regardless of their prior experience with such forms.
Follow the steps to complete the form online seamlessly.
- Press the ‘Get Form’ button to access the form and open it for editing.
- Begin filling out the member information section. Provide your social security number, date of birth, and select your status (active, retired, COBRA, survivor, or LTD). Include your last name, first name, middle initial, address, work and home telephone numbers, and the health plan name.
- Indicate your prescription drug coverage status by checking 'Yes' or 'No'. Attach copies of all health plan identification cards as instructed.
- If applicable, answer whether there is additional coverage by selecting 'Yes' or 'No' and list all other coverages, including Medicare coverage. Include the insured ID number, plan name, and employer or sponsor details.
- Proceed to the patient information section if the patient is not the member. Fill out the required patient details including their social security number, date of birth, relationship to the member, and their condition's relation to the claim.
- Complete the claim information section by providing the dates of service, the place of service, CPT/HCPCS procedure codes, diagnosis codes, units, and charges for each service rendered.
- If an itemized statement is not provided, ensure to fill in all necessary information in this section. Include the provider's name, address, federal tax ID, license number, degree, and their telephone number.
- Sign and date the member/patient’s signature and release section. Confirm that all information is accurate and complete, as the member's signature is necessary for processing the claim.
- Review the completed form thoroughly for accuracy before saving your changes. Use the options available to download, print, or share the completed form.
Submit your documents online to ensure prompt processing of your claims.
The Management Benefits Fund is funded primarily through contributions by the City of New York and employee premiums. This funding structure enables the MBF to maintain robust and sustainable benefits for retirees. By completing the MBF SMMP Claims Fax Number Form, you can easily submit your claims and enjoy the financial support that the fund offers.
Industry-leading security and compliance
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.