Get Cobra Continuation Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Cobra Continuation Form online
The Cobra continuation form is designed for individuals wishing to apply for continued health coverage after qualifying events. This guide provides step-by-step instructions on how to accurately complete the form online, ensuring you provide all necessary information for your application.
Follow the steps to complete the Cobra continuation form online.
- Click 'Get Form' button to obtain the form and open it in the editor.
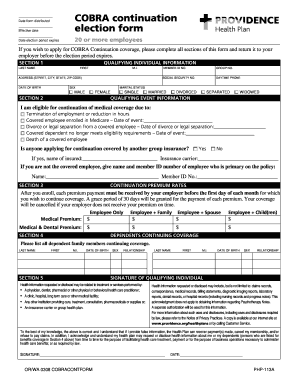
- In section 1, provide your qualifying individual information, including your last name, first name, middle initial, group number, social security number, address, member ID number, daytime phone number, date of birth, and sex.
- In section 2, indicate your marital status and select the qualifying event that applies to you, such as termination of employment or legal separation. Provide any relevant dates as prompted.
- If applicable, answer whether anyone applying for continuation is covered by another group insurance. If yes, provide the name of the insured and the insurance carrier.
- In section 3, review the continuation premium rates for different coverage options. Ensure you understand the rates for employee-only and family coverage.
- In section 4, list all dependent family members who will continue coverage. Include their last name, first name, middle initial, date of birth, sex, and relationship to you.
- Provide your signature in the designated area confirming that the information you provided is accurate. Enter the date of signing as well.
- Once all sections are completed, review the form for accuracy. You can then save changes, download, print, or share the form with your employer.
Take action now and complete your Cobra continuation form online to ensure your health coverage is maintained.
To apply for COBRA continuation coverage, you must complete the COBRA continuation form provided by your employer. After a qualifying event, you typically have 60 days to submit the form. Ensure you send it to the designated person or address specified in your COBRA notice, as this step is crucial for maintaining your health insurance coverage during the continuation period.