Loading
Get Gl3524e 15900
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Gl3524e 15900 online
Filling out the Gl3524e 15900 form for supplementary health and hospital insurance claims is a straightforward process. This guide will walk you through each section of the form, ensuring you have all the necessary information to complete it accurately.
Follow the steps to successfully complete your form.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
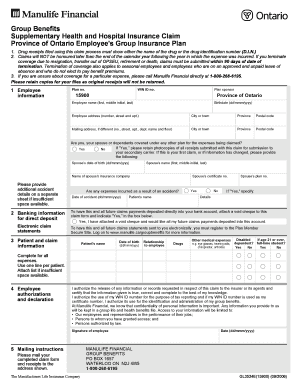
- Fill in your employee information. Start with the plan number (15900) and your WIN ID number, followed by your name including first, middle initial, and last name, along with your birthdate in the format dd/mmm/yyyy. Provide your current address including street number and apartment number, city, province, and postal code.
- If your mailing address is different, provide the details for that address in the corresponding fields, including street number, apartment number, city, province, and postal code.
- Indicate whether you, your spouse, or dependents are covered under any other plan by selecting 'Yes' or 'No.' If 'Yes,' make sure to keep photocopies of all receipts submitted for your secondary carrier.
- If this is your first claim or if your information has changed, enter your spouse’s date of birth, name, and the name of their insurance company. Additionally, provide their certificate number.
- Complete the section regarding expenses incurred due to an accident if applicable. Indicate 'Yes' or 'No' and provide the date of the accident and any patient name details.
- For direct deposit of claims payments, attach a void cheque and select 'Yes' in the provided box. Also, if you want to receive electronic claim statements, ensure you register at the specified site.
- In the patient and claim information section, fill in the patient's name, date of birth, and their relationship to you. Provide details for any drugs or medical expenses being claimed, using one line per patient and attaching a list if needed.
- Authorize and declare that all information given is true by signing and dating the authorization section.
- Finally, mail your completed claim form and receipts to the specified address for Manulife Financial Group Benefits. Be sure to keep copies for your records.
Complete your Gl3524e 15900 form online today for a swift claims process.
To fill in an expense form, choose the right form that suits your needs, such as those offered by uslegalforms. Input accurate details regarding the expenses, including the date, description, and amount spent. Always double-check your information and attach any required receipts to avoid delays in reimbursement, particularly for Gl3524e 15900.