Loading
Get Power Mobility Device Evaluation Patient Information ... - Tafp - Tafp
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Power Mobility Device Evaluation Patient Information form online
This guide is designed to assist users in accurately completing the Power Mobility Device Evaluation Patient Information form. By following the steps outlined below, individuals can ensure that all necessary information is provided clearly and completely.
Follow the steps to successfully complete your evaluation form.
- Press the ‘Get Form’ button to access the Power Mobility Device Evaluation Patient Information form and open it for editing.
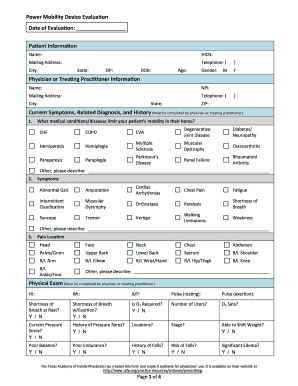
- Begin by entering the patient's personal information, including their name, health insurance claim number (HICN), mailing address, and telephone number. Make sure to fill in these details accurately to avoid any processing delays.
- Indicate the patient's gender by selecting 'M' for male or 'F' for female as needed.
- Provide the physician or treating practitioner's details, including their name, national provider identifier (NPI), mailing address, and contact number. This information should be reflective of the medical professional overseeing the evaluation.
- In the current symptoms, related diagnosis, and history section, detail any medical conditions or diseases that limit the patient’s mobility at home. Select from the provided list or add additional conditions as necessary.
- Describe the patient's symptoms from the options listed. Be as specific as possible and include any additional symptoms not covered in the list.
- Document the location of any pain the patient may experience. Use the provided body diagrams or list specific areas where pain is present.
- Complete the physical exam section by entering the patient’s height, weight, blood pressure (B/P), resting pulse, and responses to questions regarding shortness of breath, oxygen requirements, and history of pressure sores.
- Provide a comprehensive list of medications the patient is currently taking that relate to their need for a power mobility device.
- Detail the patient's functional ambulatory limitations, including gait or walk pattern and any functional limitations that apply.
- Complete the ambulatory status questions regarding the patient's ability to accomplish mobility-related activities of daily living (MRADL) safely and independently.
- Answer the mobility determination questions, indicating whether a cane or walker meets the patient’s mobility needs, and describe any necessary conditions that warrant a power mobility device.
- Finalize the form by having the physician or treating practitioner review and sign the document, certifying that all information is accurate. After making any necessary adjustments, do not forget to save your changes.
- Once completed, download the form, print it for physical records, or share it with the relevant healthcare providers electronically.
Ensure accurate documentation by completing the Power Mobility Device Evaluation Patient Information form online today.
Power chairs allow steering with just a person's fingertips. Hands and arms are also supported at all times on a power chair. Electric scooters are controlled with handlebars, or “tillers,” which require more upper body strength. This is because the tiller/handlebars must be able to be held for extended time periods.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.