Loading
Get Subscriber Statement Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Subscriber Statement Form online
Filling out the Subscriber Statement Form online can be straightforward if you follow the right steps. This guide will provide you with clear, step-by-step instructions to help ensure your form is completed correctly and efficiently.
Follow the steps to fill out the Subscriber Statement Form
- Click the ‘Get Form’ button to access the Subscriber Statement Form and open it in your chosen editor.
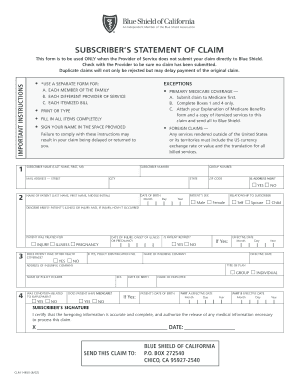
- Enter your personal information in the Subscriber Information section, including your full name, subscriber number, address, group number, city, state, and zip code. Make sure to indicate if your address is new.
- Input your date of birth and indicate the name of the patient, their sex, and your relationship to the subscriber (self, spouse, or child).
- Briefly describe the patient's illness or injury and specify how the injury occurred, if applicable. Also, enter the date of the injury or the onset of the illness or pregnancy.
- Answer whether the patient has other health coverage and if they are retired. If applicable, provide the policy identification number and the effective date of the other coverage, along with the name and address of the insuring company.
- Indicate if the condition was related to employment. If the patient has Medicare, provide their date of birth and the effective dates for Part A and Part B.
- Sign your name in the provided space, certifying that the information is accurate and complete. Include the date of signing.
- Finally, review the form for completeness and accuracy. Once satisfied, you can save changes, download, print, or share the form as needed.
Complete your Subscriber Statement Form online today for efficient processing of your claim.
Claims should be submitted to Blue Shield of California via the Real-Time Claims web tool or electronically using Electronic Data Interchange, though they can also be submitted by mail.