Loading
Get Delaware Sb1 Physician''s Report Of Wc Injury Form 2016-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Delaware SB1 Physician's Report Of WC Injury Form online
Filling out the Delaware SB1 Physician's Report Of WC Injury Form is a crucial step in documenting a worker's compensation injury. This guide provides comprehensive instructions to assist users in completing the form accurately and efficiently online.
Follow the steps to successfully complete the form.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
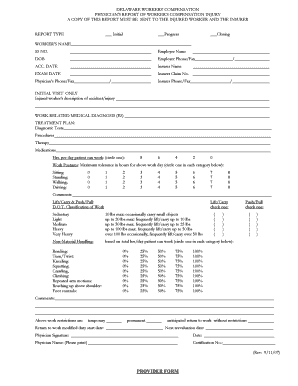
- Select the report type at the top of the form – choose between 'Initial', 'Progress', or 'Closing' to indicate the purpose of the report.
- Fill in the worker’s name, social security number, date of birth, employer name, and employer phone/fax number in the designated fields.
- Enter the accident date and the insurer's name, along with the insurer claim number in the respective sections.
- Record the exam date and provide the physician's phone/fax number as well as the insurer phone/fax number.
- If this is an initial visit, detail the injured worker’s description of the accident or injury in the available space.
- Specify the work-related medical diagnosis or diagnoses accurately in the provided field.
- Outline the treatment plan, including diagnostic tests, procedures, therapy, and medications in the relevant sections.
- Indicate how many hours per day the patient can work by circling the appropriate number: 8, 6, 4, 2, or 0.
- For work postures, circle the maximum tolerance in hours for sitting, standing, walking, and driving.
- Check the box that corresponds to lift/carry responsibilities and specify the D.O.T. classification of work that applies.
- For non-material handling, circle the percentage of time required in bending, twisting, kneeling, squatting, crawling, climbing, repeated arm motions, reaching, and using foot controls.
- Provide any necessary comments in the comments section.
- Indicate whether the work restrictions are temporary or permanent, and if anticipated return to work without restrictions is expected.
- Enter the return to work modified duty start date and the next reevaluation date.
- Lastly, have the physician sign and date the form, printing their name and certification number.
- Once completed, the form can be saved, downloaded, printed, or shared as needed.
Complete your document online today to ensure accurate reporting of worker's compensation injuries.
The Form 43 is to be completed by the respondent (employer/workers' compensation insurance carrier) to notify the Administrative Law Judge, the claimant (employee/decedent), and all parties to the claim of its intention to deny the compensability of all or part of the claimant's claim to workers' compensation benefits.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.