Loading
Get Via Benefits Forms 2020-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Via Benefits Forms online
The Via Benefits Forms allow you to manage your recurring premium reimbursement requests efficiently. This guide provides detailed instructions on each section of the form to help you navigate the process seamlessly.
Follow the steps to complete your form accurately.
- Press the ‘Get Form’ button to access the form and open it for editing.
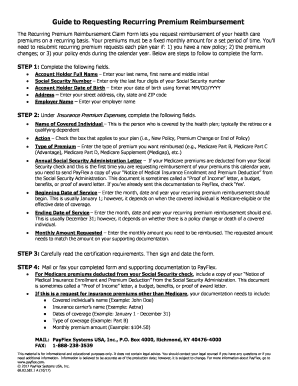
- Complete the following fields: - Account Holder Full Name: Enter your last name, first name, and middle initial. - Social Security Number: Enter only the last four digits of your Social Security number. - Account Holder Date of Birth: Enter your date of birth in MM/DD/YYYY format. - Address: Provide your street address, city, state, and ZIP code. - Employer Name: Include the name of your employer.
- Under Insurance Premium Expenses, fill out the following fields: - Name of Covered Individual: Specify the person covered by the health plan, typically the retiree or a qualifying dependent. - Action: Check the box that aligns with your situation (e.g., New Policy, Premium Change, or End of Policy). - Type of Premium: Indicate the type of premium you wish to be reimbursed (e.g., Medicare Part B, Medicare Part C, etc.). - Annual Social Security Administration Letter: If applicable, send a copy of your "Notice of Medical Insurance Enrollment and Premium Deduction" if this is your first reimbursement request for the calendar year. - Beginning Date of Service: Enter the start date for your reimbursement, typically January 1. - Ending Date of Service: Enter the end date for your reimbursement, typically December 31. - Monthly Amount Requested: State the monthly amount you seek, ensuring it matches your supporting documentation.
- Review the certification requirements, then sign and date the form.
- Mail or fax your completed form along with supporting documentation to PayFlex: - For Medicare premiums: include a copy of your "Notice of Medical Insurance Enrollment and Premium Deduction". - For other insurance premiums: documentation must include the covered individual’s name, insurance carrier’s name, dates of coverage, type of coverage, and monthly premium amount. - Mail to: PayFlex Systems USA, Inc., P.O. Box 4000, Richmond, KY 40476-4000. - Fax to: 1-888-238-3539.
Start filling out your Via Benefits Forms online today to ensure your reimbursement requests are processed smoothly.
To submit a claim to Via Benefits, start by accessing your account online or completing a paper claim form available on their site. Fill in the Via Benefits Forms with accurate details of your expenses. Attach all required documentation, and submit it online or through postal mail. Following these steps will help you navigate the claims process smoothly.