Loading
Get Medical Status
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Medical Status online
This guide provides a comprehensive overview of filling out the Medical Status form online, ensuring that you have the necessary information and steps to complete it accurately. By following these instructions, you can effectively provide the required medical information for planning services and care.
Follow the steps to successfully complete the Medical Status form online.
- Press the ‘Get Form’ button to access the Medical Status form and open it in your preferred editor.
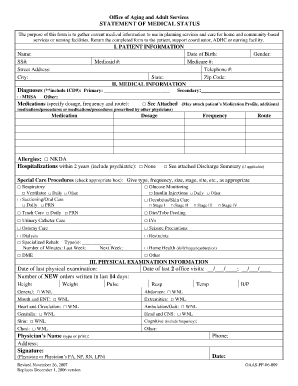
- Begin with section I, 'Patient Information.' Fill in the patient's name, social security number, street address, city, Medicaid number, state, and zip code. Ensure all information is correct and current.
- Proceed to section II, 'Medical Information.' Start with the primary diagnosis; include the ICD9 code if applicable. Specify any other conditions and provide details on medications, including dosage, frequency, and route of administration.
- Provide the patient's date of birth, Medicare number, and telephone number. Indicate the patient's allergies, hospitalizations within the last two years, and any special care procedures that need to be documented.
- In section III, 'Physical Examination Information,' document the date of the last physical examination and the number of new orders written in the last 14 days. Fill in the patient's height, weight, pulse, and other relevant physical examination details.
- Complete the remaining fields related to the patient's general condition and the physician’s details. Ensure the physician's name, address, signature, and phone number are correctly entered.
- Once all sections are filled out accurately, review the entire form for any missed or incorrect information. Save changes to your document, then choose to download, print, or share the form as necessary.
Begin filling out your Medical Status form online today to ensure proper care planning.
The content of a medical report typically includes patient identifiers, a summary of the medical status, diagnostic tests, and treatment outcomes. It may also feature notes on follow-up care and recommendations for further evaluation. A comprehensive report is vital for ensuring continuity of care and assists in informed decision-making.