Loading
Get Dhcs 6168 Spanish Forms 2020-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Dhcs 6168 Spanish Forms online
This guide provides step-by-step instructions on how to effectively fill out the Dhcs 6168 Spanish Forms online. By following these comprehensive directions, you can ensure that your form is completed accurately and efficiently.
Follow the steps to successfully complete the Dhcs 6168 Spanish Forms.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
- Begin by filling out the date in the designated field at the top of the form. Ensure that you enter the correct date as this information is crucial.
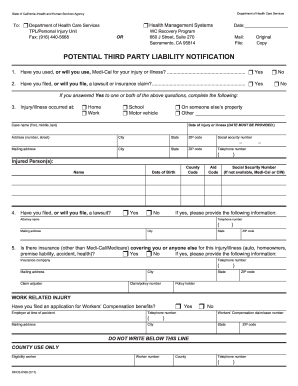
- In the Potential Third Party Liability Notification section, indicate whether you have used or will use Medi-Cal for your injury or illness by selecting 'Yes' or 'No'.
- Next, specify if you have filed or will file a lawsuit or insurance claim. Again, select 'Yes' or 'No'.
- If you answered 'Yes' to the previous questions, complete the section detailing where the injury or illness occurred by selecting the applicable option.
- Fill in your personal information including the case name, date of injury or illness, address, city, state, ZIP code, and social security number.
- Provide your telephone number in the specified format.
- If required, fill out the injured person’s details including their name, county code, and date of birth.
- Indicate if you have filed a lawsuit by selecting 'Yes' or 'No', and if 'Yes', provide your attorney's name and contact information.
- Address any additional insurance information by stating whether there is other insurance coverage for the injury or illness and providing the relevant details if applicable.
- Complete the section regarding Workers’ Compensation by providing your employer's name, Workers’ Compensation claim number, and other necessary information.
- Review all the information entered for accuracy. Once satisfied, save your changes, then choose to download, print, or share the form as needed.
Start filling out your Dhcs 6168 Spanish Forms online today to ensure timely processing of your claims!
The primary insurance program administered by DHCS in California is Medi-Cal. Medi-Cal offers health care services to eligible individuals and families, providing financial assistance for medical needs. If you require Dhcs 6168 Spanish Forms, these documents are essential for enrolling or updating information in the Medi-Cal program. They ensure that Spanish-speaking residents receive the support they need.