Loading
Get Provider Roster Template
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Provider Roster Template online
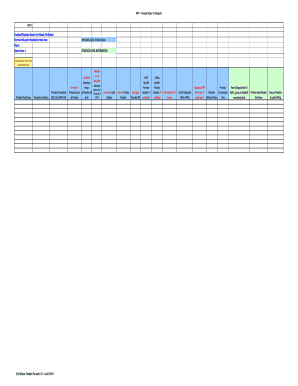
The Provider Roster Template is an essential document for managing provider-level and practice-level information. This guide will help users navigate the online form, ensuring all necessary fields are completed accurately and efficiently.
Follow the steps to complete the Provider Roster Template online
- Click the ‘Get Form’ button to access the template and open it in an online editing environment.
- Begin by entering the provider's first name and last name in the designated fields.
- Input the provider's credentials (e.g., MD, DO, APRN, PA) in the appropriate section.
- Specify the primary scope of practice and, if applicable, the secondary scope of practice for the provider.
- Select the primary care or specialist indicator by marking whether the provider is a PCP, specialist, or both.
- Provide the provider's email address and phone number for communication purposes.
- Enter the individual provider National Provider Identifier (NPI) and any available specific provider numbers from MVP or CIGNA.
- Complete the tax information section, including the individual tax ID number and any relevant PIN or PTAN information.
- Fill in the details of the parent organization if the practice is a Federally Qualified Health Center (FQHC), group, or hospital-owned practice.
- Provide the primary care practice site name and billing name for the practice.
- Indicate the affiliation type of the practice, such as group, independent, hospital-owned, or FQHC.
- Enter the complete physical address of the practice, including city, state, and zip code.
- If applicable, specify the effective date for FQHC certification.
- List the practice specialty and/or sub-specialties as required.
- Provide the practice or group NPI for payment along with the tax ID, indicating whether it is a Social Security Number (SSN) or Employer Identification Number (EIN).
- Complete the billing contact information, including first and last names as well as the billing address details.
- Ensure that the contact information for electronic funds transfer (EFT) is filled out accurately.
- If different, enter the contact information for reports, including both name and email address.
- Provide Medicare-related information such as Part A provider number and any applicable PTAN for Part B.
- Finally, review all entries for accuracy and completeness, then save your changes, download, print, or share the completed form as needed.
Start filling out the Provider Roster Template online today to ensure your provider information is accurate and up to date.
Educating patients about their health and providing relevant information about diseases and treatments. Counseling patients about their health and giving appropriate advice when applicable. Diagnosing and treating illnesses based on the presenting symptoms and relevant guidelines.