- US Legal Forms
- Form Library
- More Forms
- More Multi-State Forms
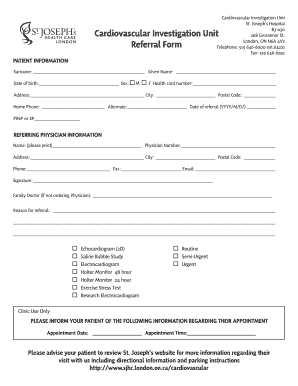
- Canada St. Josephs Health Care London Cardiovascular Investigation Unit Referral Form 2012
Get Canada St. Josephs Health Care London Cardiovascular Investigation Unit Referral Form 2012
PATIENT INFORMATION Surname: Given Name: Date of birth: Sex: M F Health card number: Address: City: Postal Code: Home Phone: Alternate: Date of referral (YYYY/M/D/): PIN# or J# REFERRING PHYSICIAN INFORMATION Na.
How It Works
-
Open form follow the instructions
-
Easily sign the form with your finger
-
Send filled & signed form or save
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Referral Related content
-
Transitional Care from Hospital to Cardiac...
by C Flores-Sandoval · 2023 — Cardiac rehabilitation is a comprehensive program...
Learn more -
Access to Heart Failure Services in Canada
by N Moghaddam · 2023 — Significant gaps and geographic variation in delivery and...
Learn more -
A RAndomizeD Intervention for Cardiovascular and...
RADICAL PC2 will test a systematic approach to modifying cardiovascular and lifestyle risk...
Learn more -
Transitional Care from Hospital to Cardiac...
by C Flores-Sandoval · 2023 — This study aimed to explore the perspectives of older...
Learn more -
Cardiovascular problems associated with aviation...
Armed Forces ECG Laboratory, Cardiovascular Unit, University Hospital,. London, Ontario...
Learn more -
Access to Heart Failure Services in Canada
by N Moghaddam · 2023 — Significant gaps and geographic variation in delivery and...
Learn more -
t1502833-s1a - block - 7.7267726s
If this Form is filed to register additional securities for an offering pursuant to Rule...
Learn more -
A RAndomizeD Intervention for Cardiovascular and...
RADICAL PC2 will test a systematic approach to modifying cardiovascular and lifestyle risk...
Learn more -
Dynamic CT Perfusion for Functional Assessment of...
A type of clinical study in which participants are identified as belonging to study groups...
Learn more -
Dynamic CT Perfusion for Functional Assessment of...
Dynamic CT Perfusion for Functional Assessment of Coronary Artery Disease ; Study Type :...
Learn more -
cardiology emergency room: Topics by ...
... Cardiology Department Unit of the San Giovanni Addolorata Hospital in Rome. In...
Learn more -
Application 6/1/2021
Jun 1, 2021 — Applicant(s) [Provide for each applicant (refer to Part 1130.220)]. Exact...
Learn more -
SAMHSA TIP 35 Enhancing Motivation for Change in...
The Treatment Improvement Protocol (TIP) series contributes to SAMHSA's mission by...
Learn more -
d/b/a Swedish Issaquah to Operate an Adult...
Application submission must include: • One electronic copy of your application...
Learn more -
Application 6/1/2021
Jun 1, 2021 — Applicant(s) [Provide for each applicant (refer to Part 1130.220)]. Exact...
Learn more -
queryResult
I am requesting all the recent inspection records (Form 483 observations) for Catalent...
Learn more -
***********Nr**************************************************...
by F NO · 1979 — administrakion of health care deliVery at.ECH. An analysip of staffing...
Learn more -
ANNUAL INSTITUTIONAL PROFILE September 1, 2011
Sep 1, 2011 — As a statewide health, education and research resource, UMDNJ benefits...
Learn more -
Approved H-1B Petitions (Number, Salary, and...
Petitions approved in a fiscal year may be filed in previous fiscal years. Per USCIS best...
Learn more -
providers
140 Ground St. 07-531, 11/30/2023, White Plains, NY, Maricopa, (480)635-1110 ... BAYADA...
Learn more -
...
Department of Health Services Research, Management and Policy. The department's...
Learn more -
2023 Annual Medical Student Abstract Journal
Oct 16, 2023 — Our hypothesis is that patients with low musculoskeletal health literacy...
Learn more -
ALISON M. STUEBE, MD, MSc, FACOG
Screening and Referral for Social Determinants of Health: Maternity Patient and Health...
Learn more -
College of Pharmacy and Health Sciences
Jan 12, 2023 — The programs leading to the Master of Science degree are designed to...
Learn more -
The COVID-19 Pandemic and Coronary Angiography for...
The COVID-19 Pandemic and Coronary Angiography for ST-Elevation Myocardial Infarction, Use...
Learn more -
Fall 2023 - Graduate Bulletin
Application for admission to the Graduate School is made to a specific program for a...
Learn more -
Ellen Keeley, MD, MS - Cardiovascular Medicine
Dr. Keeley is a professor of medicine in the Division of Cardiovascular Medicine at the...
Learn more -
6/1/23; 9:26 AM - Center for Bioethics and Health...
Jun 1, 2023 — Interprofessional team meetings in the pediatric cardiac intensive care...
Learn more -
Calendar of Events - mcw obgyn - Medical College...
Have you ever witnessed events that challenged professionalism but didn't speak up or...
Learn more -
Undergraduate Bulletin 2021–2023
Jun 4, 2023 — This is your official guide to academic policies and regulations at St...
Learn more -
Intervention Research: Designing, Conducting...
Childhood obesity is a significant problem nationwide, but certain subgroups are at higher...
Learn more -
Transitional Care from Hospital to Cardiac...
by C Flores-Sandoval · 2023 — This study aimed to explore the perspectives of older...
Learn more -
Access to Heart Failure Services in Canada
by N Moghaddam · 2023 — Significant gaps and geographic variation in delivery and...
Learn more -
A RAndomizeD Intervention for Cardiovascular and...
RADICAL PC2 will test a systematic approach to modifying cardiovascular and lifestyle risk...
Learn more -
Application 6/1/2021
Jun 1, 2021 — Applicant(s) [Provide for each applicant (refer to Part 1130.220)]. Exact...
Learn more -
Dynamic CT Perfusion for Functional Assessment of...
A type of clinical study in which participants are identified as belonging to study groups...
Learn more -
d/b/a Swedish Issaquah to Operate an Adult...
Application submission must include: • One electronic copy of your application...
Learn more -
2022 annual report | table of contents
The healthcare industry union reported $5.726 million in lobbying compensation and...
Learn more -
queryResult
I am requesting the Form 483(s), the Establishment Inspection Report(s), and any response...
Learn more -
ANNUAL INSTITUTIONAL PROFILE September 1, 2011
Sep 1, 2011 — As a statewide health, education and research resource, UMDNJ benefits...
Learn more -
Approved H-1B Petitions (Number, Salary, and...
Petitions approved in a fiscal year may be filed in previous fiscal years. Per USCIS best...
Learn more -
Intervention Research: Designing, Conducting...
Childhood obesity is a significant problem nationwide, but certain subgroups are at higher...
Learn more -
ATSDR's Annual Amyotrophic Lateral Sclerosis ...
Cardiovascular Disease. HBM. Health Belief Model. HHS. (Department of) Health and Human...
Learn more -
Consensus on diagnosis and management of ...
Lancet Diabetes Endocrinol 2021. Published Online. October 20, 2021...
Learn more -
Chronology of Events Relating to Rajneeshpuram...
This is a verbatim account of Roshani's document, with some modifications to simplify...
Learn more -
Access to Heart Failure Services in Canada
by N Moghaddam · 2023 — Significant gaps and geographic variation in delivery and...
Learn more -
The Status of Specialized Ambulatory Heart Failure...
by SA Virani · 2020 · Cited by 16 — Canada is uniquely poised to undertake this survey...
Learn more -
A RAndomizeD Intervention for Cardiovascular and...
RADICAL PC2 will test a systematic approach to modifying cardiovascular and lifestyle risk...
Learn more -
Cardiovascular problems associated with aviation...
*ment of National Health & Welfare, Ottawa, Ontario, Canada and the. Armed...
Learn more -
t1502833-s1a - block - 7.7267726s
If this Form is filed to register additional securities for an offering pursuant to Rule...
Learn more -
Dynamic CT Perfusion for Functional Assessment of...
A type of clinical study in which participants are identified as belonging to study groups...
Learn more -
Cardiovascular problems associated with aviation...
*ment of National Health & Welfare, Ottawa, Ontario, Canada and the. Armed ... Figure 1...
Learn more -
SAMHSA TIP 35 Enhancing Motivation for Change in...
The Treatment Improvement Protocol (TIP) series contributes to SAMHSA's mission by...
Learn more -
Application 6/1/2021
Jun 1, 2021 — Applicant(s) [Provide for each applicant (refer to Part 1130.220)]. Exact...
Learn more -
Office of the Whistleblower
By posting a Notice for a particular case, we are not making any determinations either...
Learn more -
...
Department of Health Services Research, Management and Policy. The department's...
Learn more -
College of Pharmacy and Health Sciences
Jan 12, 2023 — The programs leading to the Master of Science degree are designed to...
Learn more -
2023 Annual Medical Student Abstract Journal
Oct 16, 2023 — Our hypothesis is that patients with low musculoskeletal health literacy...
Learn more -
Fall 2023 - Graduate Bulletin
Application for admission to the Graduate School is made to a specific program for a...
Learn more -
Dis-Orientation Guide - Medical Student Admissions
Welcome to Washington University's School of. Medicine! As you prepare to enter the next...
Learn more -
Undergraduate Bulletin 2021–2023
Jun 4, 2023 — This is your official guide to academic policies and regulations at St...
Learn more -
Calendar of Events - mcw obgyn - Medical College...
Have you ever witnessed events that challenged professionalism but didn't speak up or...
Learn more -
Daphne M. Beingessner, M.D.
Dr. Daphne Beingessner is a graduate of University of Waterloo in Ontario, Canada and the...
Learn more -
ALISON M. STUEBE, MD, MSc, FACOG
Screening and Referral for Social Determinants of Health: Maternity Patient and Health...
Learn more -
Ellen Keeley, MD, MS - Cardiovascular Medicine
Dr. Keeley is a professor of medicine in the Division of Cardiovascular Medicine at the...
Learn more -
ATSDR's Annual Amyotrophic Lateral Sclerosis ...
Cardiovascular Disease. HBM. Health Belief Model. HHS. (Department of) Health and Human...
Learn more -
Pan-Canadian Development of Cardiac Rehabilitation...
The Canadian Cardiovascular Society (CCS) is implementing the Canadian Heart Health...
Learn more -
Intervention Research: Designing, Conducting...
Childhood obesity is a significant problem nationwide, but certain subgroups are at higher...
Learn more -
Find A Doc Data Sheet Form for Community Providers
The following form is for providers at Upstate Community Hospital who are not employees to...
Learn more -
Consensus on diagnosis and management of ...
Endocrinology Unit, Hospital. General de Catalunya,. Barcelona, Spain (E Valassi MD);...
Learn more -
QUEST FOR QUALITY IN CANADIAN HEALTH CARE
by BC VANCOUVER — At St. Joseph's Health Centre in London, Ontario, a Radiology Quality...
Learn more -
Untitled
... Care Award and Certificate|John Rowe, The Foundling Wheel (Stahlecker ... Health...
Learn more -
Building on Values: The Future of Health Care in...
Nov 1, 2002 — The contribution of the health research community to this effort has been...
Learn more -
Chronology of Events Relating to Rajneeshpuram...
This is a verbatim account of Roshani's document, with some modifications to simplify...
Learn more -
...
Department of Health Services Research, Management and Policy. The department's...
Learn more -
Recruitment Strategies in the Action to Control...
These important medical practice and public health questions are to be addressed by the...
Learn more -
Vineet Inder Chopra MBBS, MD
07/2017 – Present Co-Director, Health Services Research Unit, Divisions of General...
Learn more -
Journal of Healthcare, Science and the Humanities
General Information. In cooperation with the Smithsonian Institution Scholarly Press, The...
Learn more -
Syncope: Risk Stratification And Clinical Decision...
by SYG Peeters · 2014 · Cited by 13 — In patients with true syncope, attempt to...
Learn more -
Pan-Canadian Development of Cardiac Rehabilitation...
The Canadian Cardiovascular Society (CCS) is implementing the Canadian Heart Health...
Learn more -
Endovascular Proximal Forearm Arteriovenous...
by CE Lok · 2017 · Cited by 140 — Background: Hemodialysis arteriovenous fistulas...
Learn more -
Ellen Keeley, MD, MS - Cardiovascular Medicine
Dr. Keeley is a professor of medicine in the Division of Cardiovascular Medicine at the...
Learn more -
Syncope: Risk Stratification And Clinical Decision...
by SYG Peeters · 2014 · Cited by 13 — A prospective study of 280 patients with...
Learn more -
Find A Doc Data Sheet Form for Community Providers
The following form is for providers at Upstate Community Hospital who are not employees to...
Learn more -
Journal of Healthcare, Science and the Humanities
... St. Joseph's Health Care, London, Ontario, and as Assistant Professor in the...
Learn more -
Vineet Inder Chopra MBBS, MD
07/2017 – Present Co-Director, Health Services Research Unit, Divisions of General...
Learn more -
Author Manuscript
by E Butler · 2019 · Cited by 46 — Scleroderma renal crisis (SRC) is a...
Learn more -
...
Department of Health Services Research, Management and Policy. The department's...
Learn more -
CURRICULUM VITAE - USF Health - University of...
Division of Cardiology and Physiology & Biophysics, Mt. ... “IKs: Probing the...
Learn more -
maren theresa scheuner, md, mph, facmg curriculum...
Nov 5, 2010 — Areas of expertise/Research interests. Health services and policy research...
Learn more -
Intervention Research: Designing, Conducting...
Childhood obesity is a significant problem nationwide, but certain subgroups are at higher...
Learn more
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.
Keywords relevant to Canada St. Josephs Health Care London Cardiovascular Investigation Unit Referral Form
- yyyy
- sjhc
- echocardiogram
- ext
- Electrocardiogram
- cardiovascular
- directional
- referral
- surname
- Postal
USLegal fulfills industry-leading security and compliance standards.
-

VeriSign secured
#1 Internet-trusted security seal. Ensures that a website is free of malware attacks.
-

Accredited Business
Guarantees that a business meets BBB accreditation standards in the US and Canada.
-

TopTen Reviews
Highest customer reviews on one of the most highly-trusted product review platforms.
Select the version you need from the drop-down list below.
-
2023 Canada St. Josephs Health Care London Cardiovascular Investigation Unit Referral Form
-
2020 Canada St. Josephs Health Care London Cardiovascular Investigation Unit Referral Form
-
2012 Canada St. Josephs Health Care London Cardiovascular Investigation Unit Referral Form

